

Trial coordinator Eric McDade assesses participant Marty Reiswig for cognitive ability.Credit: Matt Miller/Washington University School of Medicine
Every two weeks, a nurse visits 43-year-old Marty Reiswig in Denver, Colorado, and injects him with an experimental drug called gantenerumab. Every month, Reiswig drives into town for a brain scan to make sure the drug has not caused any bleeds. And every year he flies to St Louis, Missouri, for four days of brain scans, spinal taps, blood analyses and exhaustive tests of his memory and reasoning capacity.
Reiswig is fit and healthy and runs two local businesses. He goes through all of this because he has a rare genetic mutation that almost guarantees he will develop early-onset Alzheimer’s disease. He hopes that the international clinical trial he has been part of for nine years might prevent, or at least delay, the onset of symptoms that will otherwise arise in just a few years’ time.
“I always do my best to give the researchers as much as I can — even if it turns out not to help me, it might help my children,” he says.
The trial is one of several trying to understand whether treating the root cause of Alzheimer’s before symptoms start might be the best way to handle a disease that exacts such a large toll. The drugs under scrutiny are all antibodies that have been developed to target and clear amyloid-β proteins in the brain, which clog together into toxic masses called plaques (see ‘Antibodies against amyloid’). These drugs are of the same type as aducanumab, made by Biogen in Cambridge, Massachusetts, which was provisionally approved last year by the US Food and Drug Administration (FDA) for the treatment of mild Alzheimer’s, in large part owing to its ability to remove amyloid-β.
And because such toxic proteins are a feature of several types of dementia, these antibody studies might also offer hints for how to treat the 55 million people around the world who have these conditions, says neurologist Paul Aisen at the University of Southern California in San Diego, who is a leader of the US Alzheimer’s Clinical Trials Consortium. Most dementias hit after 65 years of age; all have proved to be stubbornly incurable. Of more than 100 trials around the world, most are aiming to treat symptoms of the disease rather than its root cause.
But Aisen foresees a future — maybe just a decade or so down the line — in which much of the burden of Alzheimer’s disease might actually be prevented. “We’re heading towards screening people from middle age on with blood tests, and treating those who show amyloid abnormalities with drugs that reduce the generation of amyloid plaques,” he says. “I am optimistic.”

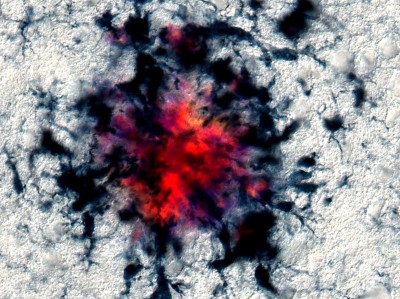
PET (positron emission tomography) scans of the brain of a person with Alzheimer’s show the build-up of amyloid plaques (circled) not present in healthy brains.Credit: Science Source/SPL
A lot needs to go right for this hopeful view to become reality. Large clinical trials will have to show that these therapies work, and amyloid-clearing drugs will have to be proven to be safe and affordable. After decades of setbacks and failed clinical trials, some dementia researchers prefer to express caution. “The field is taking tremendous risks by engaging in studies that can cost billions of dollars,” says neurologist David Knopman at the Mayo Clinic in Rochester, Minnesota.
It will take a while for answers to emerge. Some trials of Alzheimer’s disease prevention are just getting started, and some ongoing ones could stretch into the next decade.
Getting in early
It was 1986 when Carol Jennings in Nottingham, UK, wrote a letter to geneticist John Hardy asking whether she could be of use in his research. Just like Reiswig, Jennings had many relatives who succumbed to early-onset dementia. Hardy’s team, now at University College London, was interested in the genetics of Alzheimer’s and invited the Jennings family to donate blood to its project.
A few years later, the team identified a mutation shared by the affected family members1. It was in a gene that codes for a large protein that sits in the membranes of neurons, the amyloid precursor protein (APP).
APP in the brain is chopped into amyloid-β and other short chains of amyloid protein by a suite of enzymes. In healthy brains, these amyloid peptides might serve useful functions, but over time they can accumulate — perhaps because the brain’s molecular system for clearing them loses efficiency — and clump together into plaques. In someone with a mutation in the gene that codes for APP, the amyloid-β proteins are stickier or more profuse, and the disease manifests earlier than in people who do not have the mutation.
This is the basis of the amyloid hypothesis of Alzheimer’s disease, first formulated by Hardy and his colleagues after their discovery of a disease-causing APP mutation. According to that theory, preventing the triggering event of amyloid-β accumulation might slow the disease process — or even stop it happening in the first place.
Is ‘friendly fire’ in the brain provoking Alzheimer’s disease?
Pharmaceutical and biotechnology companies set about targeting the amyloid system, developing drugs to block the enzymes that cleave APP, or creating antibodies to the amyloid-β peptides. But their drugs continuously bombed in clinical trials. Five phase III clinical trials of a drug that blocks an amyloid-chopping enzyme, β-secretase, were discontinued because of side effects that made cognition temporarily worse. Blockers of another enzyme, γ-secretase, went the same way. Time and time again, trials of antibodies designed to latch onto and bind to amyloid-β failed to improve people’s clinical symptoms. At least one major pharmaceutical company, Pfizer, left the Alzheimer’s field, in 2018.
The serial failures divided the research community into camps. One camp argued that if targeting amyloid hadn’t worked, then the amyloid hypothesis must be wrong. Knopman accepts that APP processing is part of the disease initiation process, but says that the role of amyloid-β has not been proved. “It’s plausible, for example, that other APP cleavage products are more important to the disease process,” he says.
The other camp argued that the trials had been poorly designed, in particular because they recruited people who had already begun to show early signs of Alzheimer’s disease.
“The fact is that, to optimize the potential impact of removing amyloid, you need to do so as early as possible,” says Aisen. Amyloid-β accumulation begins its slow and silent campaign of destruction in the brain many years before its damage is extensive enough to cause symptoms, he says. “The total duration of Alzheimer’s disease is over 25 years, and the trials were only engaging in the final decade when there is constant worsening of neurodegeneration.”
Animal studies back up this insight. In mice that were genetically altered to overexpress APP, treating young animals with aducanumab before amyloid-β deposits were detectable resulted in significant reductions in deposits and fewer signs of disease in the brain six months later2.
When the FDA made the controversial decision to approve Biogen’s aducanumab in June last year, it was recognizing this long-term picture: that the drug’s ability to remove amyloid-β made it likely that it could reduce Alzheimer’s symptoms down the line. Biogen’s large, placebo-controlled trials of aducanumab in people with mild Alzheimer’s had not unambiguously improved their clinical symptoms, but the drug did a good job of clearing amyloid plaques from their brains. The agency declared that aducanumab was the first treatment to affect the biological cause of the disease.
The decision enraged many researchers who claimed that the FDA had lowered its standards. (Knopman resigned from the FDA’s advisory committee over this issue.) But in the following months, more data emerged from other trials of different drugs, showing trends towards a modest slowing of cognitive decline as amyloid-β was cleared, as well as reductions in other biomarkers of Alzheimer’s progression, such as the build-up of a protein called tau. Later that year, the agency put three further antibodies onto a fast-track review process: Genentech–Roche’s gantenerumab, Biogen–Eisai’s lecanemab and Eli Lilly’s donanemab. Similarly to aducanumab, all three have been shown in early trials to clear plaques.

Credit: Nik Spencer/Nature
“These drugs are big, big game changers,” says neuroscientist Bart de Strooper, director of the UK Dementia Research Institute at University College London. “They will allow the amyloid hypothesis to be tested definitively.”
Many researchers agree that the best test of the hypothesis — and the best way to stop the disease in its tracks — is to give people these drugs early, without waiting for Alzheimer’s symptoms to set in first.
Timing is everything
According to Hardy, designers of even the earliest trials might have realized that they were recruiting too late in the disease. “Through the retrospectoscope, it was clear — the data were already there,” he says. In the 1980s, pathologist George Glenner at the University of California, San Diego, and his colleagues discovered that individuals with Down’s syndrome developed dementia relatively young3. They suggested that this was because people with Down’s syndrome have an extra chromosome 21 (where the APP gene sits). Their post-mortem studies4 showed that plaques developed many years before cognitive symptoms did.
The field is not ignoring the importance of finding treatments for symptomatic Alzheimer’s, says Aisen. But clinical researchers are now turning more attention to drug trials for the treatment of presymptomatic Alzheimer’s disease. It is not easy to find participants for such trials, however. People need to be symptomless but highly likely to begin developing symptoms on a measurable timescale. There are two approaches to identifying these individuals: find people like Reiswig with a rare genetic predisposition, or people in the general population with a high risk of developing Alzheimer’s because of the presence of amyloid-β in their brains.
Landmark Alzheimer’s drug approval confounds research community
To identify the rare genetic cases, the US National Institute on Aging (NIA) in Bethesda, Maryland, funded the launch of the Dominantly Inherited Alzheimer Network (DIAN) in 2008. It now includes more than 600 people from 20 countries, representing around 300 families who have mutations in one of the three genes associated with early-onset Alzheimer’s. Each family member has a 50% chance of inheriting a mutation.
The network quickly gathered more funding and research partners, and began enrolling families, including Reiswig’s, into an observational programme. The researchers conducted positron emission tomography (PET) scans of the brain to check for amyloid-β and other biomarkers of Alzheimer’s at regular intervals, and compared family members who carried the gene with those who didn’t. They also noted when symptoms tended to begin in each family. The network’s 2018 report confirmed that the first signs of amyloid abnormalities occur up to 25 years before symptoms start5.
The DIAN consortium began a seven-year trial of amyloid-binding antibodies in 2012. It aimed to delay the progress of disease in people who have no cognitive symptoms but who have started to develop the primary markers of Alzheimer’s — amyloid plaques — in their brains. The trial recruited 194 participants at various stages of their condition, and divided them into groups to receive either one of two antibodies, gantenerumab or solanezumab, or a placebo.
But the results of the trial, announced in 2020, were disappointing. The trial failed to prove that the drugs could slow cognitive decline — although there was little decline in treated presymptomatic participants, there was also little decline in the placebo group6. “That meant that we were simply unable to say whether the drugs would eventually help an asymptomatic population or not,” says Randall Bateman at Washington University School of Medicine in St. Louis, who leads the DIAN Trials Unit that conducted the study.
Still, one of the antibodies, gantenerumab, had a notable impact on the biological markers of the disease. It not only reduced amyloid plaques, but also reduced levels of tau protein and of another marker of neurodegeneration, a neuronal protein that shows up in the blood.
These results encouraged Bateman and the DIAN consortium to continue studying gantenerumab for a further three years, dropping the solanezumab and placebo arms but allowing participants in those groups to convert to gantenerumab, and letting them know what drug they were taking.
That presented Reiswig with a dilemma. When he was originally tested for the gene mutation, he had chosen not to be informed of the result. But the extension of the study was only available to mutation carriers, so a request to participate would automatically reveal his genetic status. “I decided it was time for me to know, but I planned things carefully,” he says. He retreated to a holiday rental in Colorado with his wife to receive the phone call from his genetic counsellor. “I didn’t want to find out in my own house — that was at least something I wanted to have control over.” Reiswig wept when he learnt that he carried the mutation, and decided that his only chance was to continue with the trial.

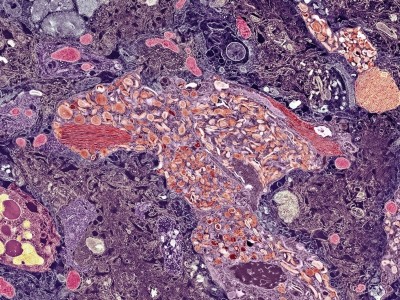
An amyloid plaque (centre) in the brain tissue of a person who had Alzheimer’s disease.Credit: Martin M. Rotker/SPL
Last year, the consortium decided to try treating people with no cognitive symptoms and no plaques in their brains. “It’s really going to be the ultimate trial of Alzheimer’s prevention,” says Bateman. In the next few months, the team plans to begin recruiting 160 mutation carriers, some as young as 18, who are not expected to develop symptoms for another 11–25 years. The placebo-controlled trial will run for four years, monitoring people’s amyloid status at regular intervals. Then it will move into an ‘open label study’ for a further few years: the placebo arm will be dropped and all the participants will receive the trial drug. At that point, it will also measure other biomarkers of disease progression.
It would be impractical to run the trial for the decades it might take for participants to develop symptoms, says Eric McDade, the trial’s principal investigator at Washington University in St. Louis. Instead, the team will monitor changes in biomarkers, such as amyloid-β and tau, that are now known to predict symptom onset during the long silent period of the disease. “The more of these other biomarkers that we can alter, the higher the probability that we can offset or at least significantly delay onset.” The researchers will continue to monitor as many participants as possible after the trial’s second phase, he says.
Outside the DIAN consortium, other trials for early-onset Alzheimer’s are under way, testing drugs in people who already have some amyloid build-up. Genentech–Roche is studying individuals from a large family in Colombia, half of whom carry a pathological mutation in a gene that encodes part of one of the amyloid-chopping secretase enzymes. Its trial of the drug crenezumab will finish this year. Studies are also gearing up to test Alzheimer’s drugs in people with Down’s syndrome.
Stopping symptoms
The second approach to preventive trials is to identify those in the general population who are at high risk of developing late-onset Alzheimer’s. The international Alzheimer’s Disease Neuroimaging Initiative, a public–private partnership headquartered at the University of California, San Francisco, tracks Alzheimer’s biomarkers in many hundreds of people through normal ageing and all stages of the disease. Its data show that around one-third of cognitively normal people aged over 65 have amyloid plaques in their brains, and that more than 85% of them will go on to develop symptoms of Alzheimer’s within 10 years7.
On this basis, three large, placebo-controlled clinical trials are under way, each recruiting more than 1,000 people who are cognitively fit but have brain plaques, as seen by PET scanning. Each trial is testing a different antibody. All three will run for four years, by which time cognitive decline is usually measurable after plaques begin to accumulate.
The red-hot debate about transmissible Alzheimer’s
Aisen’s institute is coordinating the A4 trial — Anti-Amyloid treatment in Asymptomatic Alzheimer’s — which is testing the Lilly drug solanezumab. Results are expected next year. Aisen also co-leads the AHEAD 3-45 trial, which began in 2020 and is testing lecanemab. That same year, Lilly started a trial called-Alz 2 with donanemab. And this year, Roche is launching its own phase III trial with gantenerumab, which will run for sixyears.
The costs of such trials “is typically hundreds of millions of dollars”, says Aisen. Just recruiting the 1,169 participants in the A4 trial required around 4,500 PET scans, each costing an average of US$7,000. “But costs to society of this disease in terms of suffering, mortality and economic impact justify enormous investments in effective treatment,” he says.
In recent years, there has been substantial progress in developing simpler, blood-based biomarkers of Alzheimer’s disease. Two of these prevention trials are using such biomarkers to help select people for PET screening, chipping away at the cost of PET scans and the inconvenience for participants. One biomarker measures the ratio of two slightly different forms of amyloid-β, and another measures a tau-related molecule.
So far, the preventive trials all use antibodies against amyloid-β. These drugs have two disadvantages. They can have side effects: small brain bleeds or swellings, which are mostly harmless, but which can be serious. And they are expensive. Biogen initially fixed its price of a year’s treatment with aducanumab at $56,000, although it halved it in December 2021.
But the field is thinking about revisiting simpler, small-molecule drugs, which would be much cheaper to produce than antibody-based therapies. Some companies are starting to consider revisiting the secretase enzymes, says Aisen, perhaps tweaking the structure of the enzyme-blocking molecules that failed in early trials, or finding better ways to administer them.
Complex causes
Researchers in the field are aware that addressing dementia also requires an effort beyond amyloid-β. “Alzheimer’s disease is more complex,” says neurobiologist Roger Nitsch, one of the original developers of aducanumab at the University of Zurich, Switzerland. “Amyloid is a very slow-burning neurotoxin which initiates the disease, but brain cells — including those connecting to blood vessels and cells of the immune system — fight back.” There will be more ways to target established disease, he says. Also, only around two-thirds of all dementias are of the Alzheimer’s type, and post-mortem studies show that half of these have mixed pathology —the brains contain other toxic proteins in addition to amyloid and tau, or signs of blood-vessel damage8.
Prevention trials are important and promising, says NIA director Richard Hodes, “but we are not giving up on people who already have disease”. Because there will probably be multiple contributors to dementia — even in the same individual — a range of treatments will be needed, he says. The NIA is funding 72 clinical trials for dementia, trialling drugs aimed at various targets. Some, for example, aim to lower blood pressure to reduce the risk of small blood vessels breaking in the brain; others target tau. Only 20 target amyloid. The NIA is also supporting at least 120 trials to study the impact of non-pharmacological interventions, such as cognitive training, exercise and diet.
Researchers estimate that, in 2021, a total of at least 126 different agents — including those in NIA studies — were being investigated in clinical trials around the world9.
As a volunteer, Reiswig has had to accept the special burden that his particular trial brings — not just the time commitment, but also the constant reminders of the fate that awaits him if the trial drug doesn’t work. It helps, he says, that the DIAN consortium brings participants from all over the world together once a year to share their experiences. “We’ve created a wonderful community and we know we contribute strongly to science.”
Nature 603, 216-219 (2022)
doi: https://doi.org/10.1038/d41586-022-00651-0
References
-
Goate, A. et al. Nature 349, 704–706 (1991).
-
Uhlmann, R. E. et al. Nature Neurosci. 23, 1580–1588 (2020).
-
Glenner, G. G. & Wong, C. W. Biochem. Biophys. Res. Commun. 122, 1131–1135 (1984).
-
Ikeda, S., Yanagisawa, N., Allsop, D. & Glenner, G. G. Lab. Invest. 61, 133–137 (1989).
-
Gordon, B. A. et al. Lancet Neurol. 17, 241–250 (2018).
-
Salloway, S. et al. Nature Med. 27, 1187–1196 (2021).
-
Donohue, M. C. et al. JAMA 317, 2305–2316 (2017).
-
Kapasi, A., DeCarli, C. & Schneider, J. A. Acta Neuropathol. 134, 171–186 (2017).
-
Cummings, J., Lee, G., Zhong, K., Fonseca, J. & Taghva, K. Alzheimers Dement. 7, e12179 (2021).